
A History of Birth in the United States
This is a paper that I wrote back in 2013 — during my university years — that I still stand behind. It’s not my usual casual language and there’s zero playfulness. It’s all academic, all serious, and all gigantic paragraphs (ugh). But it’s such an important topic and I need to start sharing some of the research I’ve done over the years, so I’m starting here.
I’ve bolded some elements of the paper for ease-of-skimming (for those of you who find academic writing boring), and I’ve added some photos and visual elements to support the content and make it more interesting to look at. 😉
Additionally, this is A history of birth… There are many, many histories of birth, midwifery, medicine that can be told from many perspectives. I would like to attempt to capture many other historical perspectives in future posts. This is one perspective, with a focus on how the experience of gender impacts the development of an industry such as obstetrics.
I hope you get a lot out of it — enjoy!
Throughout the last century, human childbirth was fraught with an underlying clash of power due to perceptions about gender. The experience of gender is marked by profound differences in many societies, something that is also found in American culture. Birth is just one of those experiences, but for many it can have a deep, lifelong impact on how they view themselves and the world around them. A social construct of gender can influence how a woman is treated from the point of sexual education, if there is any, to the experience of raising a child. During the last century, childbirth in America has undergone considerable change. It has transformed from a woman-centered, at-home affair attended by female midwives to a medicalized experience away from all that is familiar, controlled mainly by professional men.
Stone carving from Göbekli Tepe, 9500-8000 BCE (source)
Prehistorically, birth was an experience that had very few choices, as compared with today. One made-do with what was available, the end goal being simply survival and the hope of a healthy mother and child. The difference in choice arrived with cultural constructs surrounding birth, each human group arranging their prescriptions and taboos according to their own practical and spiritual worldviews. Choices then varied based on how a society viewed women’s roles and what was considered appropriate conduct within that role. One culture might allow a woman to express each aspect of her birth, while another might discourage this and instead encourage a face of silent bravery. In some societies, a woman would give birth surrounded by others, yet in another she would venture off to give birth alone. Some birthing styles brought about higher mother and infant mortality, others were more successful in saving the lives of the birthing dyad. In many ancient societies, it seems that the feminine was a central theme and as a result, women were often given more power, autonomy, and prestige. Women more often directed their own fertility routines and rituals, with consideration of the male role, but through a culture of female positivity. In her book The Control of Childbirth: Women versus Medicine through the Ages, Phyllis L. Brodsky describes this earlier time:
The history of childbirth embodies the history of women and how they were viewed through the ages. In the beginning women were highly valued; they were regarded as the supreme race among the sexes. They were the goddesses, the queens and the designated healers. The goddesses represented the heavens, the earth, nature, fertility, birth, and death. It was mainly women who originally discovered the earth’s bounty and its healing properties. (13)

Roman stone carving (source)
As time continued, however, an almost universal shift occurred that rendered women subordinates of men, stripped of much of their autonomy and power. They found ways to preserve their dignity, however, and many female-centered cults emerged as a result. Traces of this experience can be seen in modern-day religions, as in the worship and following of the Mother Mary in the Christian tradition.
Leading up to the industrial revolution, western women were generally oppressed and seen as a lesser gender. Much medieval literature and educational movements were directed at portraying women as vile, filthy, and deceptive. The very tale from the Bible of Adam and Eve casts the female in the role of an untrustworthy being who is incapable of choosing what is perceived as ‘right.’ This was the deeply embedded belief system that impacted every aspect of a colonial, and then Victorian, woman’s life. Her entire existence was constructed to contain this supposed inherent ‘evilness’ that was not under her control. Women who achieved a high state of spirituality, through fasting, celibacy, and the like, were revered as saintly and having overcome the “female curse.” It is necessary to understand this cultural construction in order to perceive the evolution of childbirth during this era.

Sheela na gig (source)
At the beginning of this time period, birth was still in the hands of other women (Leavitt 87). A kind of female kinship was formed that allowed women to have support networks during this often difficult time. Midwives were the authorities on the subject of female reproductive functions and the healers in the world of women. Physicians were gaining popularity, as science became a sweeping trend, but many taboos existed that would not allow them full entrance into the world of female “mysteries.” Many rituals and traditions were in place at that time that could cause infection, pain, and ultimately death for one or both birthing parties, mother and child. Birth was perceived as a painful, dangerous affair for many women. It is important to stress that many more women experienced birth as a safe, uneventful occurrence, but the prevailing cultural mentalities surrounding gender and the human animal experience had a profound effect on the cultural experience.
Physicians initially were called in when a birth went awry and surgical help was deemed necessary. Very quickly, however, they realized that they knew very little about female reproductive anatomy and even less about birth. Some midwives were kind enough to patiently demonstrate appropriate care of a mother in labor, and slowly male physicians were able to integrate obstetric care into their surgical practices (Leavitt 59). The movement of science afforded doctors the ability to invent tools that might better assist in a birth emergency. The most commonly known tool being the forceps (Brodsky 46).
Many Victorian era women were afraid of their bodies, malnourished, and uncomfortable with being reduced to what they perceived as a lowly animal during the messy birth process (Leavitt 67). Having men present in the room during such a physical experience, already a staunch taboo, made them behave in ways that invoked a clinging to female modesty as much as possible. This meant many women gave birth fully clothed, with nearly everything covered unless an article of clothing was absolutely necessary to remove (Leavitt 40-42). Birth became a process that was experienced lying down, instead of the previous method of the mother moving in whatever way lessened the discomfort. Women felt a greater need to refrain from expression, and so they attempted to maintain a dignified social face in the presence of what must have felt like ‘the public’ and ‘the stranger.’ This very behavior exacerbated birthing pain, leading to a need for great assistance to remain ‘in control’ while lying down in the prone position. Physician-attended births thereby brought about a kind of physical and mental pain not known previously, at least not in as common of an occurrence. This fear experience brought about a state of fight-or-flight that made birth very difficult. Therefore, use of forceps became almost a necessity, and pain medication became sought after with a fervor. Medical science promised better outcomes for women, pain relief, and emergency help when things went wrong. As resistant as a woman might have felt due to social taboos, many women wanted physicians to attend their births, and many of the upper-class that could afford to pay for a medical birth would (Leavitt 109-10). The first medicines that allowed some sort of relief from pain were touted far and wide by the women who used them. This experience was seen as providing options for women, and in a time of serious gender oppression was also perceived as advancement and a ‘good thing’ for all women.
Initially, women clung to their female circles for support during labor, birth, and the postpartum period (Leavitt 97-98). Midwives were still very much present at births, as they knew the most about the normal birth process and remained the experts (Brodsky 67). But physicians became more commonly associated with births as well. The progressive, and typically higher-class, woman aligned herself with social, political, and educational progress, and medicalized birth was placed squarely in the midst of this.
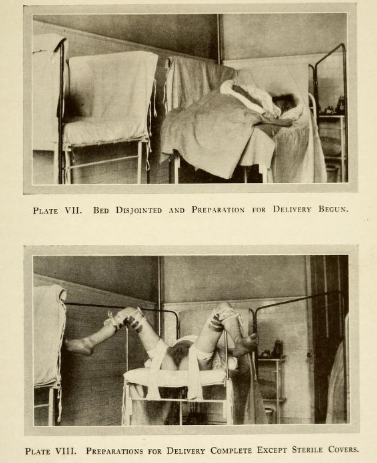
In the early part of the 1900s, the majority of women still gave birth at home. A great number of those births were physician attended, complete with surgical tools, pain management, and remedies. Very quickly, however, birth moved to the hospital. Physicians realized early on in their care involvement that as long as they were in the women’s homes surrounded by their peers, family members, and care providers, they were only allowed to be there to assist and could not orchestrate control over the experience. They were not in their own environment, therefore could not act as the authority in a space that was traditionally female dominated (Leavitt 102-05). An early priority for the medicalization of childbirth was to get the women into a space with which a doctor was avidly familiar: the surgical unit, otherwise known as the hospital. In this place, he was the authority and could make demands which were carried out without question. Once women moved their births to the hospital, they were suddenly confronted with an environment very unlike anything they were familiar with. Family members were not allowed in the room, and the women were in a strange place, with strange authority figures, strange tools, and embarking on a taboo experience of which they knew very little. It became the perfect condition for complete control over birth. In Brought to Bed Childbearing in America, Judith Walzer Leavitt states:
Much of childbirth history reflects a debate between tradition, defined culturally, socially, and temporally, and a slowly developing rational model of science. Women frequently found themselves at odds with impersonal science as represented by the medical birth attendant, but at the same time they were attracted by the promises of science. They wanted what both worlds had to offer. (208)

Early hospital-based obstetrics (source)
Drugs had made their grand entrance into the world of childbearing at this point. Chloroform and ether were commonly used, most especially by those who could afford the excessive cost: women of the upper-class. In fact, it was believed that their class of women should most especially be given anesthesia because they were more prone to “nervous tendencies” (Leavitt 126). One such doctor's description of his typical upper-class patient from 1893:
We all know that the pregnant woman is prone to having her nervous system out of joint; in fact, the condition in itself is a severe test to the female nervous system…during the entire term the imaginations of the woman often becomes exalted or depressed. Her disposition is irritable… Suspicion, jealous, general sensitiveness are present, which under other conditions are never dreamed of. Nervous pains abound, migraine, facial neuralgia, toothache, itching in various parts of the body… The most grave nerve troubles sometimes are present... Truly we have evidence in favor of the thought that pregnancy is a severe test to the stability of the nervous system (Leavitt 126).
Anesthesia became something offered out of compassion for a laboring woman, but also because it made the job of caretaker much easier for the doctor. It is difficult to care for a person who is experiencing an extreme amount of pain, and it was felt that if another option existed, why on earth would they not offer such a remedy?
Twilight Sleep (source)
Within a few decades, drugs and anesthesia became commonplace. The chloroform and ether of the previous era became replaced by something called twilight-sleep. This was a combination of harsh narcotic drugs that left a mother half-awake, but entirely unaware of her surroundings. Women were placed into crib-like beds for their own safety, and tied down so as to not harm themselves or their baby (Wolf 52, Leavitt 129). When they awoke from the drugged state, a baby would suddenly appear by their side, which produced the odd effect of feeling as though they could not be sure if this was truly their child, having no recollection of the birthing experience. This method was hailed as an incredible remedy to the pain experienced in birth and became ubiquitous. However, as Leavitt explains: “Women's bodies experienced their labors, even if their minds did not remember them. Observers witnessed women screaming in pain during contractions, thrashing about, and giving all the outward signs of 'acute suffering'” (128-29). Twilight-sleep became a tool of the women's suffrage movement (Leavitt 137). It was seen as an advancement in medical science and something that would allow women to escape the mold of enduring what was seen as a Biblical curse. It gave women options and choices, and the illusion of safety in science. They were more than willing to give up their support group of women at home in order to embrace that which seemed more logic-based (Leavitt 174-75). They believed that previous generations of women had not had many choices, and the demands of pain medication were perceived as for the rights of choice among women. On the physicians' side of things, this new movement was seen in a slightly different light:
...[the physicians] stood on the brink of increasing their power over birth processes, but in 1914 they did not yet have the control they desired over procedures and decisions... The vehemence of the medical argument about lay interference thus is attributable to this state in the development of obstetrics when physicians were beginning to understand the possibility of ultimate control without yet experiencing the reality of it... (Leavitt 138-39).
By the 1930s, it was realized that, regardless of the advancements, hospital birth was just as inherently dangerous as home birth had been, courtesy of the skyrocketing maternal and infant mortality rates. Safety became a serious public health concern, and officials worked to uncover why mortality rates were staying the same and often even increasing. Many otherwise healthy women went to the hospitals to give birth, but then died while there due to cross-contamination which lead to postpartum infection. Some physicians were unafraid of addressing this issue and publicly blamed medical practice for the lack of attention to extreme cleanliness that was shown in other parts of the hospitals' practices. Many doctors resisted this idea claiming that to change their practices required funding that they did not feel they could allocate to childbirth. Others discussed ethics and moral responsibility, fueling a heavy debate on adequate care for mothers and their babies (Leavitt 182-83). The majority of this debate did not reach the ears of the women giving birth, however, as the physicians “did not want to 'frighten the women too much'...” (Leavitt 189). Thankfully by the 1940s and 50s, remedies to these infections had been discovered and the maternity death rate began to decline at last (Leavitt 194).
During the process of all of this, women started to comprehend that something was missing from the birth process that they did not expect. They “...realized, perhaps too late, that the physical removal of childbirth from the woman's home to the physicians' institution shifted the balance of power... Women were no longer the main actors; instead, physicians acted upon women's bodies” (Leavitt 190). Because of the highly medical, surgical-based environment of the hospital, a woman's body became a platform for procedures instead of the dynamic space of creation of which it had always been before. They were under the patriarchal control of men in power, which is not at all what they had intended. Many women who had experienced the world of hospital birth determined to give birth at home once again, despite the advantages of a supposedly sterile environment. They were willing to take the risk in order to be in charge of their own process and to have the psychological comfort of home surrounding them. There were, of course, women who delighted in the hospital experience, enjoying the bustling about them and constant service and rest. Granted, the majority of these women were most likely those who could afford high-end hospitals which represented the upper-class experience (Leavitt 81). Those who gave birth in poverty-inflicted hospitals were in for an often misogynistic and sometimes dangerous experience (Leavitt 77). Leavitt explains the following:
Women at the middle of the twentieth century were bound in a medicalized system of birth that had evolved over the course of American history. Although they had participated in bringing about the changes, including the move to the hospital, women had not anticipated the full meaning of this last most crucial alteration. While physicians were aware of the importance of shifting locations of power, because they had been frustrated by their lack of power in women's homes, women...were less in touch with what they were leaving behind by moving to the hospital. They did not realize that in gaining what they had hoped would be safer controls over the previously uncontrollable parts of home confinements, they were giving up their ability to determine the environment of their labor (206-07).
In the decades since women fully began to realize their misfortune, a safer form of anesthesia arrived, which is still used today: the epidural. Along with it appeared the natural childbirth movement, as women began to demand a return to individual choice and autonomy over their own bodies. The first physician to promote this ideology was Dr. Grantly Dick-Read, a prolific writer about the subject. Many women grabbed hold of the concept and ran with it, declaring that women had been duped and could in fact regain their dignity through abstaining from the whole medicalization of birth altogether.

Copyright: Sarah Braun
In the last half of the twentieth century, homebirth made a comeback, and with it enormous amounts of research on the safety of hospital practices in birth and the psychological effects of such practices. Many women reported life-long trauma that directly pointed to their hospital birth experience. During this time period, cesarean sections, once a life-saving surgery, became standard practice in a growing number of normal birth situations (Brodsky 145, 167). As plastic surgery became a normalized practice, so did the scheduling of c-sections for women who simply wanted to avoid the birth process altogether. While a portion of the population of women were declaring their rights to determine their own birth experience through “natural” practices, another portion was still riding the bandwagon of pain relief in all aspects of birth. A certain demographic of women declared that the right-of-passage of women – traditionally birth – was removed, thereby causing depression and a great number of other ailments of the twenty-first century. One study found a link between post-traumatic stress disorder and the experience of a traumatic birth. Specifically, it presents an intriguing discovery in the connection between cesarean sections and PTSD. It seems that the mothers who experienced more of the symptoms of PTSD were those who gave birth by planned cesarean section, whereas these symptoms were not experienced as often by those who underwent emergency cesarean surgery or gave birth vaginally (Beck, et al 225).
It seems as though women are reclaiming autonomy in birth and reinstating the role of female comforters during labor. In the past twenty years, doulas – birth attendants that help reduce pain during labor through “natural” techniques, midwives, and other alternative practitioners have been on the rise and popularized through the use of media, literature, and old-fashioned female networking. Birthing at home and in birthing centers has also found a committed and passionate audience. A recent study reported that most developed nations have comparable rates of persons who give birth at home, that number being just under 1 percent. The Netherlands remains a bit of an anomaly, their home birth rate being at about 30 percent. The rates in England, New Zealand and the United States have all risen in a significant way in recent years. Oddly, most of these rate increases occurred at a time when home birth activism was not nearly as present as it was soon after the increase. Shortly thereafter, documentaries, articles, and international organizations were created (MacDorman, et al 189).
As I have shown in this discussion, childbirth is very much steeped in the culture of gender roles. The influence is profound and far-reaching. It is often a taboo subject as science has become an institution that is not easily questioned in medical matters. Often, women are understandably uncomfortable with the discussion simply because it calls into question their own birth choices. However, this analysis is not about which choice is better than another, but rather the influence of progressive gender equality movements and the psychology of women in relation to cultural practices.
Have cultural attitudes toward gender honestly changed since the century during which birth drastically transformed? Has medical science brought equality as adequately as it has brought infection-fighting practices? It appears that it is likely not so. For example, Emily Martin reports that in scientific literature, while it would seem that the reproductive systems in both males and females should be given equal importance, after closer inspection, it appears that adjectives and passive versus active voice come into play in a rather unequal way. Female organs are seen as creative and the beginning of menstruation as the end to that role of creation, and a loss or deficiency in ability – a kind of let-down or failure. The female menses are often described in negative terms as a sort of dying of the possibility of life. The male reproductive system, on the other hand, is often described in an awe-inspiring, positive light. It is seen in an active and assertive role, and its mysteries are lauded as incredible and life-giving (486-87). Perhaps gender norms continue to influence the ways in which women are treated in a medical setting, especially as it applies to the ways in which they are different from men, specifically in situations that deal with the reproductive system.
In conclusion, it is important to consider the influences of ancient birth practices, modern medical science, and also the natural childbirth movement of the latter half of the twentieth century. All things in a society are dynamic, with a constant ebb and flow. Could it be possible for the modern-day woman to arrive at a place with birth in which she is treated with utmost respect, accepted as an autonomous being, given whatever modern medical interventions that she feels are important, but also allowed to just be? Perhaps the United States could look to countries such as the Netherlands in which a large percentage of normal births occur at home with access to all the modern conveniences, but with the comfort of what our ancestors found so necessary: female support and companionship. Margarete Sandelowski sums up this idea well:
While Natural Childbirth promised the most happiness in the childbirth experience, virtually everyone agreed that the key variable affecting happiness was not any specific method of childbirth but rather the quality of the physician-patient relationship. Several studies demonstrated that behind every happy maternity patient, whether under the influence of drugs or Natural Childbirth, was a doctor in whom she had placed her faith and her fate. (115)
Through the perspective of the history of childbirth in America, I feel that gender roles and expectations become readily apparent. Especially when a person is vulnerable, as in the process of birth, it seems as though how that person is treated explicitly demonstrates mass social conceptions of gender. Pain produces various reactions in both the person experiencing the pain and also in those assisting that person. This transparency gives us a blatant view of gender-influenced interactions. The evolution of how and where a woman gives birth shows how gender has such a huge impact on the way in which women are treated. As we are enculturated in our own culture, these beliefs and behaviors have become normalized and are difficult for us to easily identify. However, with a little research and some comparing and contrasting, it can be eye-opening as to how extensively gender affects nearly every aspect of our lives.
Resources
Beck, Cheryl Tatano, Robert K. Gable, Carol Sakala, and Eugene R. Declercq. "Posttraumatic Stress Disorder in New Mothers: Results from a Two-Stage U.S. National Survey." Birth 38.3 (2011): 216-27. Print.
Brodsky, Phyllis L. The Control of Childbirth: Women versus Medicine through the Ages. Jefferson, NC: McFarland &, 2008. Print.
Leavitt, Judith Walzer. Brought to Bed Childbearing in America, 1750 to 1950. New York: Oxford UP, 1986. Print.
MacDorman, Marian F., Eugene Declercq, and T. J. Mathews. "United States Home Births Increase 20 Percent from 2004 to 2008." Birth 38.3 (2011): 185-90. Print.
Martin, Emily. "The Egg and the Sperm: How Science Has Constructed a Romance Based on Stereotypical Male-Female Roles." Signs: Journal of Women in Culture and Society 16.3 (1991): 485-501. Print.
Sandelowski, Margarete. Pain, Pleasure, and American Childbirth: From the Twilight Sleep to the Read Method, 1914-1960. Westport, CT: Greenwood, 1984. Print.